





Share:
The knee is a common body part for injuries in runners. The purpose of this blog post is to highlight some of the more common knee running related injuries and provide examples of knee exercises. When recovering from injury, I recommend consulting a physical therapist for specific guidance on what exercises you should be doing for your knee pain. These exercises can be performed if you are not having pain for injury prevention.
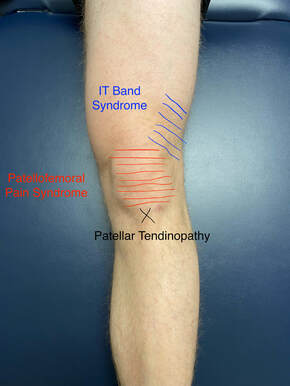
Patellofemoral pain syndrome (PFPS) aka “runner’s knee”
What is it?
Generalized term for pain around or behind the kneecap (patella) when all other diagnoses have been excluded. Pain is often exacerbated by squatting, stairs, lunging, kneeling, and running.
What causes it?
- Patellofemoral pain syndrome in runners is often from overuse and training errors. Runners tend to do too much too long or too much too soon. A spike in running volume, aka too much too soon, can cause increased stress on knee that it is not ready to handle, and the end result is pain. A gradual increase in running mileage of about 10-33% a week is recommended.
- High running mileage with adequate rest, aka too much too long, is another training error common in runners. Yes, every once in a while, you need to decrease your running volume to give your body a rest.
- If you have not made training errors resulting in overuse but are still having knee pain, then there are muscle strength, motor control, and/or flexibility deficits contributing. Even with a perfect training progression, you can still have knee pain if there are impairments in one or more of these categories.
Iliotibial band (ITB) syndrome
What is it?
Overuse injury caused by repetitive knee bending and straightening resulting in irritation to structures on the outside of the knee. It is the most common source of lateral (outside) knee pain in runners. The exact source of pain is debated. The most common explanation is from repeated flexion and extension of the knee causing friction where the ITB courses over the lateral femoral condyle resulting in inflammation and pain. Newer evidence is leading toward a fat pad under the femoral condyle that becomes inflamed and painful. Either way, repetitive flexion/extension of the knee, especially around 0-30 degrees knee flexion causes pain at the lateral knee.
What causes it?
- Overuse from an increase in running, biking, or hiking mileage. This may be obvious, but training errors are often the main culprit to ITB syndrome, especially when in conjunction with any of the below impairments.
- Flexibility deficits of the quads, hamstrings, hip flexors, tensor fascia latae, and ITB itself. Flexibility deficits can cause movement pattern impairments placing stress on the ITB.
- Strength deficits, specifically in the gluteus medius, minimus, and quadriceps. If these muscles are not doing their job, the TFL will kick in. The TFL directly attaches to the ITB, and excessive TFL activation causes increased stress to the ITB by pulling directly on it and tightening it up.
- Motor control deficits (faulty movement patterns). One example is dynamic valgus (knee jetting inward) at the knee during single limb support in running which causes increased stress on the ITB.
Patellar Tendinopathy aka “jumper’s knee”
What is it?
Tendons are load bearing structures that responsible for transmitting force from muscle to bone.Tendinopathy (more commonly referred to as tendonitis) is pain and tendon dysfunction, often with structural changes to the tendon. Some structural changes to the tendon are reversible in the early stages of tendinopathy, but tendon structure changes can become irreversible in the later stages. Even with irreversible structural tendon changes, pain and function can improve! The healthy part of the tendon remodels and strengthens to make up for the dysfunctional part of the tendon.
The patellar tendon is located at the bottom of your knee cap (patella). If the pain is from the patellar tendon, there will be localized pain to the tendon. Generalized pain to the bottom of the knee is probably not patellar tendinopathy! Also, the pain must be dependent on load (external force) and is worse with running and jumping because of the high rate of tendon loading. Running and jumping have a high rate of tendon loading because the force from the activity is transmitted to the tendon quickly. Once the tendon is irritated, it can hurt at rest, walking, or stairs.
What causes it?
Tendinopathy (anywhere in the lower body) is an overuse injury from excessive repetitive loading without adequate rest. Patellar tendinopathy has been named “jumper’s knee” because a high volume of jumping is often the cause. It is less common to have patellar tendinopathy with runners, but it does happen. The risk factors listed below may predispose someone to patellar tendinopathy, but without overuse, symptoms will likely never develop.
Risk factors:
- Running or jumping sports
- Quadriceps or hamstring tightness
- Weakness of quadriceps
- Decreased ankle range of motion
- Patella alta (anatomically higher sitting patella)
- Recent increase in training volume and/or surface
Now that I have discussed some of the more common diagnoses for running related knee pain, I will demonstrate some of the best exercises for the knee. Many of the exercises demonstrated will be squat variations. Squats variations are hands down the best exercises for knee prehab and rehab. Squats can also be one of the most provocative motions for the knee, especially if you are already in pain. A properly sequenced and dosed exercise program is needed if you experiencing pain, so please consult a physical therapist if you are unsure of how to do this on your own!
There is an abundance of misinformation on the internet about squat exercise safety and technique.. With that in mind, this article’s intention is not to be a deep dive into the squat. I’ll save that for another blog.
Now, after all that talk about squats, the first exercise shown below is not a squat but a quadriceps activation and strengthening exercise. It is a great starter exercise if you are having difficulty contracting your quadriceps or need a lower level strengthening exercise that is less irritating to the knee.
Straight Leg Raise
Okay, now to the squat variations. The wall squat with a foam roller is often less provocative to the knee than a normal body weight or goblet squat because there is less forward translation of your tibia (shin bone). If the knee hurts with other squat variations, this variation of the squat is key. I used weights in the video, but you do not need to use weights at first. Hold the squat at the bottom and feel your quads burn!
Foam Roller Wall Squat
The body weight squat is next on the list. Despite it being a common exercise, I get many questions about this exercise with my patients. Squat technique is not easy! There is also no universal way to squat, which I briefly talk about in the video. Body weight squats allow more forward transition of the tibia than the wall squat, which places more force through your knee than the wall squat.
Body Weight Squat
The goblet squat is next up and this is one of my favorite options for a more quadriceps and knee dominant squat. What I mean is the goblet squat forces your torso to be more upright, making your knees translate further forward during the squat. This produces a larger force at the knee joint and larger contribution from the quads during the exercise. At the same time, there is less stress placed on the hips and low back. I like to use this one earlier in low back and hip rehab and later in knee rehab for these reasons.
Goblet Squat
Now, I am going to transition to split pelvis movements (legs staggered with one in front of another). Split pelvis movements are great to start emphasizing strength unilaterally. Strictly bilateral movements can allow for compensations for weaker muscles. Split squats are not lunges. Split squats allow for a vertical shin angle (think the wall squats mentioned above), which can be less irritating to the knee. Lunges have more forward translation of the tibia, producing more stress on the knee. Lunges are still effective to build strength and poweras the knee becomes less irritable. I only show forward lunges in the video, but there are a myriad of lunge variations out there and all can have utility depending on the goal of the exercise.
Split Squat
Forward Lunge
In addition to bilateral and split pelvis movements, unilateral movements are important to build strength and movement control. Step downs are useful to build in the quadriceps and gluteals. The higher the step, the harder it will be on the muscles and also higher stress on the knee. People often find it challenging to balance at first, but this improves quickly and is important to work on.
Lateral Step Down
Single leg squats are a progression of a step down. You do not have to do a full pistol squat for it to be effective. Starting with tapping a high surface like shown in the video is a good way to practice working on the movement without having to worry about falling or poor technique.
Single Leg Squat
In closing, knee pain does improve with conservative care for most people. If your pain is persistent or you want more guidance, it might be a good time to contact a physical therapist!
Disclaimer: This content is designed for information & education purposes only and is not intended for medical advice.
Blog by:
Dr. Dylan Michel, PT, DPT
References
- Willy RW, Hoglund LT, Barton CJ, Bolgla LA, Scalzitti DA, Logerstedt DS, Lynch AD, Snyder-Mackler L, McDonough CM. Patellofemoral Pain. J Orthop Sports Phys Ther. 2019 Sep;49(9):CPG1-CPG95. doi: 10.2519/jospt.2019.0302. PMID: 31475628.
- van der Worp MP, van der Horst N, de Wijer A, Backx FJ, Nijhuis-van der Sanden MW. Iliotibial band syndrome in runners: a systematic review. Sports Med. 2012 Nov 1;42(11):969-92.
- Rudavsky A, Cook J. Physiotherapy management of patellar tendinopathy (jumper’s knee). J Physiother. 2014 Sep;60(3):122-9. doi: 10.1016/j.jphys.2014.06.022.
- Malliaras P, Cook J, Purdam C, Rio E. Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. J Orthop Sports Phys Ther. 2015 Nov;45(11):887-98. doi: 10.2519/jospt.2015.5987.



